

Case Studies
Examine the preop radiographs to estimate the inner diameter of the
intramedullary canal of the affected phalanges at the location where
you expect the implant’s arrow tip to engage. Determined with a ruler
and taking into consideration radiographic magnification, the inner
diameter at the point of engagement in the bone should be at least
3.5mm to ensure an effective fit, ease of insertion, and mitigation of
the possible impingement of the arrow tip upon the cortices. Use the
ruler to determine the length of ARROW-LOK™ implant that will engage
each phalanx at the intended point of contact and the broaching
depth for each phalanx.

Create a standard 3cm central incision over the surgical toe.

Dissect through the skin and subcutaneous tissues down to the extensor tendon at the deep fascial level. Perform a transverse tenotomy/capsulotomy at the dorsal crown of the proximal phalanx. Dissect and transect the medial and lateral collateral ligaments away from the bone to expose the head of the proximal phalanx into the surgical site.
Dissect the soft tissue away from the base of the intermediate phalanx, exposing the cartilaginous surface for resection and arthrodesis preparation.

Resect the head of the proximal phalanx and base of the intermediate phalanx bones. Smooth all rough edges of bone.

Create a pilot hole down the center of the intramedullary canals of both the proximal and intermediate phalanx with the ARROW-LOK Reamer.


Prepare the pilot hole on both the proximal and intermediate phalanges with the ARROW-LOK Broach.Broach each phalanx as deeply as the anatomy will permit while carefully considering the depth estimated during preop planning. Make note of the depth marking to which the broach was inserted in each phalanx.







Grasp the ARROW-LOK implant with the ARROW LOK Insertion Forceps at
the depth corresponding to the broaching depth of the proximal phalanx.

Insert the implant into the proximal phalanx, locking it into the intramedullary canal.


Grasp the digit and insert the distal aspect of the implant into the entry portal
prepared in the intermediate phalanx locking the implant into the intramedullary canal.


Release and remove the Insertion Forceps. Grasping the digit firmly, compress the two bones together to advance the implant both proximally and distally to its final and locked position.


Close the digitorum extensor longus and brevis to help further stabilize the proximal interphalangeal joint that has just been fixated with the ARROW-LOK implant. The more stable a fusion site is, the faster union takes place.


Close the wound in accordance with generally accepted surgical technique.

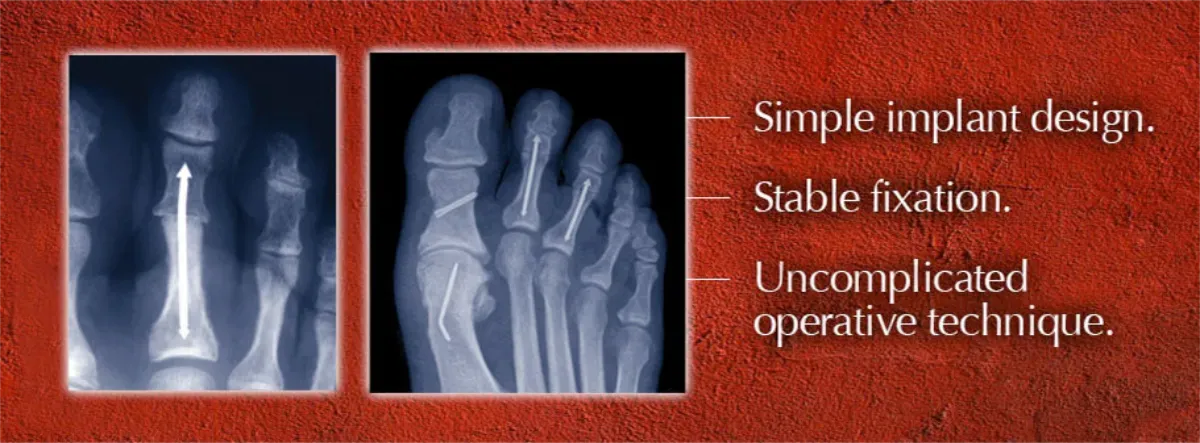
Radiographically evaluate the final positions of the implant and ensure that the proximal and intermediate phalanges are in close contact without gapping.

Attention Patients
Would you like your surgeon to use the ARROW-LOK Digital Fusion System for your hammertoe correction?
Call us at 470-419-1429 or email us and we will direct you to an ARROW-LOK surgeon.
